
Every April, Boston-area massage therapists see more than the usual amount of people with strained soleus muscles. This injury can be quite painful and last longer than most muscular injuries, and it often occurs in marathoners—especially those who run hilly courses, like Boston’s.
The soleus (Image 1) is the largest and strongest muscle in the calf. It gains its power from its complex configuration, attaching to its corresponding tendons at a 45-degree slant (called a multi-pennate structure) in multiple rows. The muscle starts at the top of the calf and attaches to the Achilles tendon at the bottom. It lies underneath the gastrocnemius muscle, which was discussed in a previous article [“Gastrocnemius Muscle Strains,” Massage & Bodywork, November/December 2010, page 90]. These two structures are intimately connected, with some of their fibers overlapping. Some people consider them to be a single muscle, but their functions are different, and different tests are needed to check for injury of either structure.
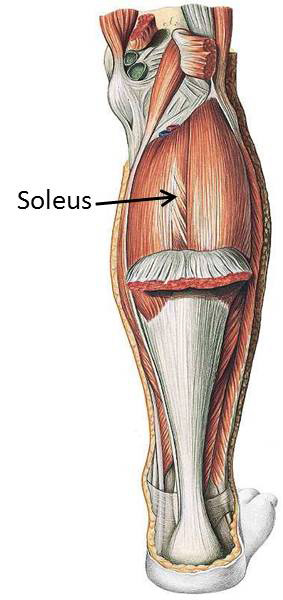
Image 1: Soleus muscle
Pain from a soleus strain is felt deep in the calf, usually in the superior part, toward the knee. Discomfort can be felt in one spot or over a broad area, because this injury can leave many fibers strained and inflamed.
How and Why This Injury Occurs
It takes a lot of stress to injure this muscle. As mentioned, running uphill is one way people strain the soleus. That’s because running uphill forces a person to bend his or her knees more than usual, and that puts a lot more stress on the soleus muscle.
This same kind of stress is experienced with a lot of high jumping. Most people don’t roll through the foot when they land from a jump, and landing on the balls of the feet with the knees bent puts stress on the soleus. If this is done repeatedly, the soleus can become compromised and ultimately injured.
Improper alignment throughout the body can also affect the soleus muscle. For instance, when the feet are pronated and the arches are dropped, more of the body’s weight is shifted toward the medial half of each foot. This places an imbalanced amount of weight on the medial half of the soleus and very little weight on the lateral half. As a result, one portion of the muscle is overused while the other is underused, causing an imbalance of muscle strength across the muscle fibers. Consequently, when force is applied to the lower leg, both halves of the muscle are vulnerable to injury—the medial half because it receives excessive strain, and the lateral half because it’s in a weakened state.
At the other end of the body, the alignment of the head and neck can also contribute to a soleus injury. If the head is forward and out of alignment, the other end of the body is forced to compensate. A continual stress is placed on the posterior aspect of the entire leg, making it more vulnerable to gradual breakdown and eventual injury.
Injury Verification
When the soleus is injured, a dull aching pain begins during, or directly after, strenuous activity. This injury isn’t usually debilitating, but it puts a stop to the strenuous activities a person might enjoy doing, like tennis, biking, or running. As the injury progresses and more adhesive scar tissue develops, the discomfort in the calf comes on with more mundane activities, like walking.
Here are three tests to perform if you suspect a soleus injury is to blame for a client’s calf pain.
Test 1. Bent-Knee Heel raises
Have the client stand barefooted with the feet parallel, shoulder-width apart. Ask the person to bend the knees as far as possible, keeping the heels firmly on the floor and the back erect. Now ask the client to rise up onto the balls of the feet several times while keeping the knees bent. If the soleus muscle is severely strained, this will cause discomfort or pain.

Bent-knee heel raises
Test 2. Single Leg Bent-Knee Heel raises
If the first test does not cause any discomfort, try this variation to increase the stress on the injured area. Have the client stand on one leg (the injured one), holding onto something for balance. Now have the person rise onto the ball of the foot, being sure to keep the knee bent.
As mentioned earlier, the soleus muscle is very strong, so this test alone may not cause pain, especially if the client has to run four miles or play tennis for 30 minutes before the calf begins to hurt. If no pain is felt, repeat the test immediately after the client performs an activity that causes pain; this time, while the leg is already aching, you’re testing to see if the discomfort increases. If this test still does not produce or increase the pain, the client may have injured the gastrocnemius muscle instead.
Test 3. Alignment Check
Have the client stand naturally, and take a good look at the alignment of the person’s feet. Well-aligned feet are parallel or rotated outward no more than 5 degrees. When the feet are pronated, the arches drop and may almost touch the floor; the feet are generally rotated 10–20 degrees laterally. Also, when the person bends the knees 2–3 inches, the knees will go straight forward while the feet point outward. To relieve the strain on the entire medial leg and prevent future damage from occurring, this type of misalignment is as important to address as the injury itself.

Alignment check
Treatment Choices
Treatment requires as much patience as there is strain: the greater the strain, the longer the healing time.
Self-Treatment, Massage, and Friction Therapy
There’s a lot people can do on their own to help the soleus. In mild cases, rest and bent-leg heel raises are sometimes effective, though this may take many months. The main danger is returning to strenuous activity too soon without slowly building up strength. Friction therapy coupled with massage can help speed the process along, enabling the healing of recent injuries within four to six weeks and more long-standing injuries within eight to 12 weeks.
To perform fiction therapy on the soleus muscle, have the client lie face down on your table. Sit on the table just below the client’s knees, and bend the knee of the affected leg to a 90-degree angle. Position the ankle on your shoulder, keeping the knee at a 90-degree angle. Wrap your hands around the calf with all of your fingertips pointed directly into the center of the calf, and with your thumb holding the shin. Sink your fingertips into the central calf so that you go through the gastrocnemius muscle and contact the soleus. While applying that anterior pressure, move horizontally, from medial to lateral, for a minute or two. Then move over to a different section of the soleus, covering all the painful areas in sequence. Do this for 5–6 minutes, rest, and then do it again. After the friction, apply massage to the calf for 4–5 minutes.
Exercise Therapy
When you treat people with soleus strains, give them the following exercises (taken from Aaron Mattes’s Active Isolated Stretching and Strengthening protocols) to do on their own. Doing them consistently, every day of the week, can greatly speed the healing process along. I’ve written the instructions as directions for the injured person to follow; you can read them to your client or give them a copy to bring home.
Stretching. Begin with a warm-up of either walking for a few minutes or extending and flexing the foot while sitting down. Next, sit on the floor and bend the knee of the affected leg to 90 degrees, with the knee facing the ceiling and the foot flat on the floor. Be sure the foot is in a straight line from the shin (not turned in or turned out). Now use your muscles to raise the forefoot off the floor as far as you can, and then wrap your fingers around the forefoot and pull gently toward the knee (see images at right). Continue to pull for 2 seconds, and then release the foot back down to the floor. Be careful not to stretch for more than 2 seconds each time.
Repeat this motion 8–10 times, and then turn the foot out and repeat the same stretch 8–10 times. Finally, repeat the stretch 8–10 times with the foot turned in.


Stretching the soleus
Strengthening the Soleus. Start by standing and rising onto the balls of the feet with knees extended (straight). The feet should be parallel and shoulder-width apart. Do three sets of 10, with a brief rest between sets. As that becomes easy, add the same exercise with the feet turned in and then with the feet turned slightly outward. Next, do the whole thing with the knees bent throughout the exercises.
Once those variations are easy to do, progress to doing the same exercise while standing with the balls of the feet at the edge of a step, so that the heels drop below the level of the forefoot. Begin with the knees extended and progress to having the knees bent throughout. The final stage of this exercise is to slowly begin to place more weight on the injured leg. The goal is to be able to do the exercise standing on one leg (the injured one), while holding onto something sturdy for balance.
These strengthening exercises don’t work the soleus muscles alone; they call on the gastrocnemius to do a portion of the work, especially when the knees are extended. As the client gets stronger, he or she can call on the soleus more by keeping the knees bent at all times throughout the exercises.
Orthotic Devices
In some instances, misalignment of the feet can be corrected by working with an exercise specialist. However, this takes a fair amount of work, self-awareness, and a really good teacher, and most clients will not put in the necessary time and effort. A simpler solution is using orthotic devices to realign the foot and take the weight off the medial calf. These can be purchased in drugstores, in shoe stores, or by mail order, but to get a high-quality device fitted precisely to the foot, it’s best to see a podiatrist who specializes in making and adjusting orthotics.
Conclusion
Injuring the soleus muscle usually requires great stress, and repairing it may require great patience. Combining friction therapy, massage, and the strengthening and stretching exercises described above can move things along more quickly; correcting any alignment problems will go a long way toward preventing the return of the problem.
Ben E. Benjamin, PhD, holds a doctorate in education and sports medicine, and is founder of the Muscular Therapy Institute. Benjamin has been in private practice for more than 45 years and has taught extensively across the country on topics including orthopedic massage, Active Isolated Stretching and Strengthening, and ethics. He is the author of Listen to Your Pain (Penguin, 2007), Are You Tense? (Pantheon, 1978), and Exercise Without Injury (MTI, 1979), and coauthor of The Ethics of Touch (Sohnen-Moe Associates, 2003). He is also offering continuing education for massage therapists around the world via webinars. He can be contacted at Ben@BenBenjamin.com.
Editor’s note: Massage & Bodywork is dedicated to educating readers within the scope of practice for massage therapy. Essential Skills is based on author Ben E. Benjamin’s years of experience and education. The column is meant to add to readers’ knowledge, not to dictate their treatment protocols.




